Easy-to-use technology, amazing orthotics and great patient outcomes from an orthotic lab you can trust
Northwest Podiatric Laboratory has invested heavily in proprietary manufacturing technologies to enhance the capabilities of its experienced craftspeople. Over the last decade, we’ve developed new 3D imaging innovations like the In-Office Foot Digitizer foot scanner and SmartCast® to help more healthcare professionals provide world-class orthotics.

SmartCast – a foot scanner using an iPad, 3D sensor and custom app – is truly a leap forward for podiatrists, foot and ankle surgeons, physical therapists and pedorthists seeking handmade quality and the ease of digital. From a practice management perspective, SmartCast is a win-win: speed and efficiency meet quality and unrivaled patient outcomes.
SmartCast and Northwest Podiatric Laboratory elevate custom foot orthoses
We get better data. Patients get better orthotics.
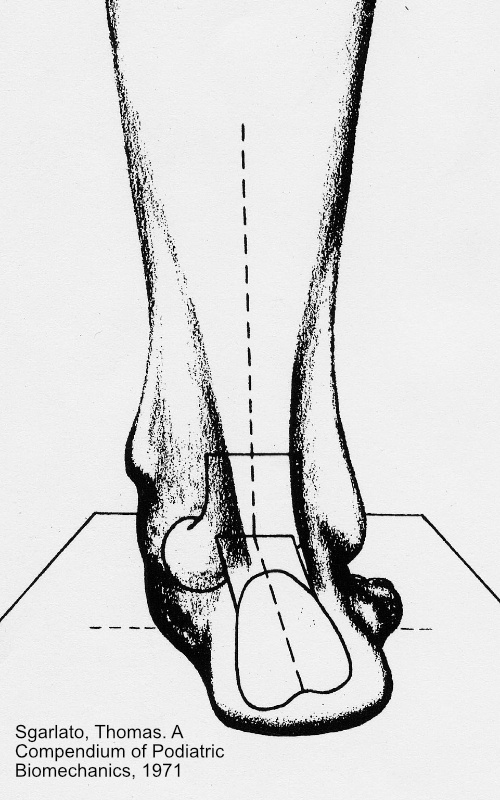
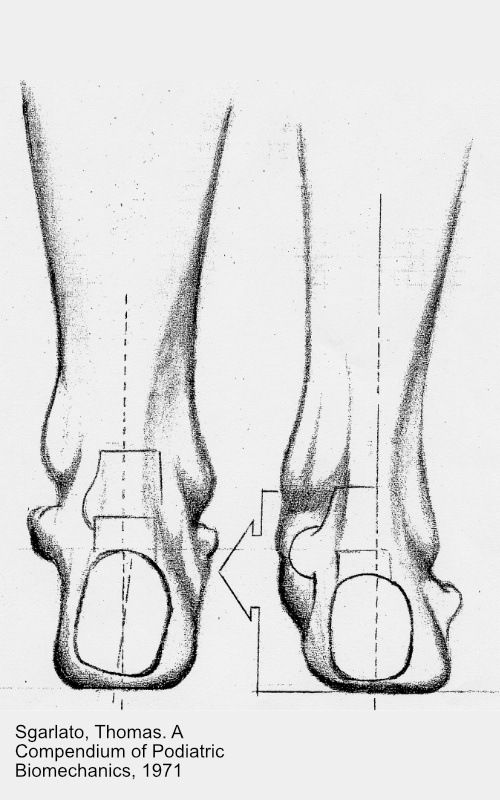
The patented SmartCast Foot Positioning System® helps healthcare professionals achieve perfect foot positioning every time. Great positioning and accurate 3D scanning ensure custom orthotics are crafted with unrivaled accuracy and function.

A superior experience.
SmartCast is quicker, more comfortable and less messy than traditional plaster casts or foam impressions. Best of all, the ease, convenience and speed don’t come at the expense of quality. With SmartCast, we’re crafting the best custom orthotics in our history.
Orthotics…faster!
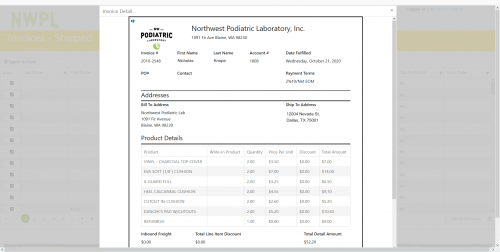
Orders for orthotics are submitted digitally and received immediately at Northwest Podiatric Laboratory – there’s no extra processing, handling or shipping time. NWPL far surpasses the industry norm by crafting and ships custom orthotics in days and not months.
Handmade in the United States by people who truly care.
Our orthotics are crafted in Blaine, WA by skilled technicians with hundreds of years of combined experience. NWPL has earned its history and experience the hard way: through decades of work and dedication. With the same ownership since 1964, NWPL doesn’t need to create or fabricate a history; nearly 60 years of authenticity is built into every pair of orthotics that hundreds of thousands of patients benefit from every day.
Go from foot pain to happy feet in four simple steps:
- Position and align the foot using the patented SmartCast Foot Positioning System®
- A 3D scan of the foot is captured and reviewed for accuracy and completeness.
- Scans and prescription information are securely submitted to NWPL and our technicians craft orthotics for each patients’ unique foot and foot pain – plantar fasciitis, bunions, heel spurs, hammer toe, Morton’s neuroma, sesamoiditis and more.
- Finished orthotics are dispensed to patients who are now ready to do what they love with one-of-a-kind custom orthotics supporting them every step of the way.
Learn more about what industry professionals are saying about scanning for custom orthotics
Podiatry Today
Is Scanning More Effective Than Casting For Custom Orthoses?
Is 3D scanning Eclipsing Traditional Casting For Orthotics?
American Podiatric Medical Association
3-D Scan or Cast for Orthotics? That is the Question.
Ready to step up to SmartCast?
Contact our knowledgeable Customer Care Team at [email protected] or 800-443-7260.
Northwest Podiatric Laboratory is an industry leader in custom foot orthotics and related technologies. Dennis Brown, a retired British soldier, elite athlete and natural-born inventor founded the company in 1964 and was joined by a pioneer in the biomechanics of the foot, Dr. Chris Smith, in 1974. With an exclusive blend of science, craftsmanship and innovation, the partners have built a company that utilizes proprietary production techniques and technology to produce orthotics with a unique shape and unparalleled performance. Northwest Podiatric Laboratory has helped over a million people suffering from foot pain to lead better, pain-free lives. Learn more at www.nwpodiatric.com.