When it was introduced in the early 1960’s, the rearfoot post was intended to invert the rearfoot of the orthotic (and the foot) a specific number of degrees enabling the subtalar joint to function around its neutral position. A rearfoot varus of nine degrees was given a varus post of nine degrees. (See Fig. 1). In theory, at heel contact the calcaneus would be inverted to the floor by nine degrees – so long as the lateral platform of the post was bearing the majority of body weight. (See Fig. 2). The subtalar joint would subsequently pronate as the weight shifted from the lateral platform to the medial platform. (See Fig. 3). The medial platform of the post was angled four to six degrees relative to the lateral post to facilitate physiologic pronation of the subtalar joint. When the medial platform was fully engaged with the supporting surface it acted as a terminal brake and subtalar joint rotation would cease. After this initial physiologic pronation ended the foot would subsequently resupinate to neutral and beyond producing a stable foot in preparation for propulsion.
This paradigm is erroneous. In the example above, when the medial platform is fully engaged in weight bearing, the distal medial aspect of the orthotic plate is five degrees inverted to the floor, a mechanical impossibility. (See Fig. 3).
With time, the high degrees of rearfoot posting steadily reduced to the customary four degrees (and sometimes 6 degrees) because of the potential for inversion sprains with the higher postings. Today, most rearfoot posts have a four degree varus lateral platform with a four degree medial grind off (See Fig. 4) to allow four degrees of rearfoot eversion at heel contact. (See Fig. 5). This means that resupination starts at the heel vertical position and is not dependent upon weight bearing of the medial platform. This change in perception requires some explanation.
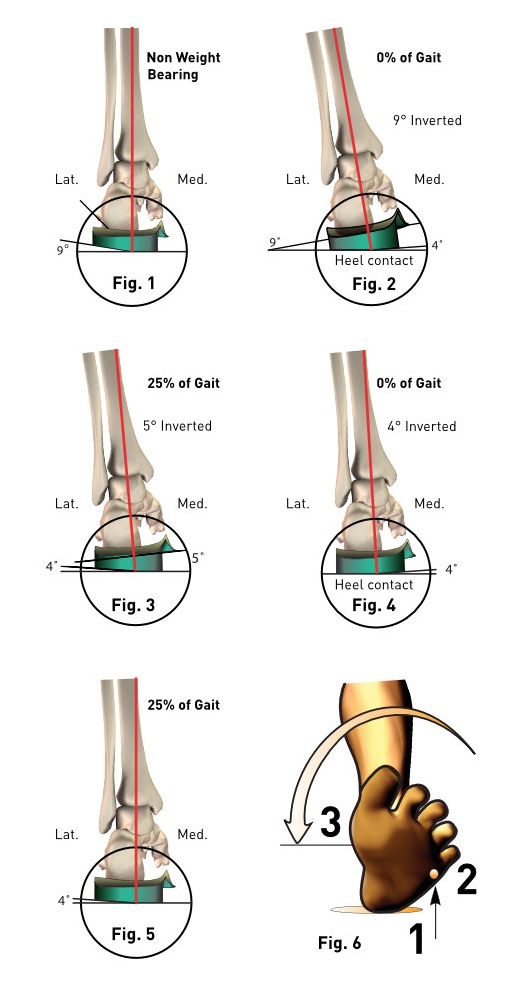
In order to understand why resupination is not dependent on the medial platform of the post but rather the vertical position of the heel, consider the foot during the first 25% of stance as the foot contacts the floor. The foot contacts the supporting surface in the following sequence: lateral heel, then lateral forefoot, then medial forefoot and finally medial heel. (See Fig. 6). Medial forefoot contact and medial heel contact are almost simultaneous. Notice that the forefoot is everted on the rearfoot (locking the midtarsal joint) by the reactive force of gravity pushing upwards through the lateral forefoot. The same sequence occurs with the functional device: lateral platform of the heel, followed by the lateral forefoot and finally, the medial platform of the post. Thus, the eversion of the forefoot on the rearfoot ultimately shifts the weight to the medial platform of the posts. The end-point of the eversion of the rearfoot is determined by the contact of the distal-medial aspect of the orthotic plate with the transverse plane and not by the medial platform engaging the supporting surface. In reality, the heel vertical position is the termination point of heel contact pronation no matter what degree of post is applied to an orthotic plate.
Increasing the value of the rearfoot post may be counterproductive. With higher degrees of posting a more inverted position is possible at the initial portions of heel contact but the subtalar joint must pronate further to reach the vertical end point. Remember the end point is determined by the distal medial aspect of the orthotic plate rather than the medial platform of the post. In other words, increasing the value of the rearfoot post increased the amount of pronation of the rearfoot at heel contact.
As stated before, most rearfoot posts will theoretically invert the rearfoot by four degrees and this is quickly followed by pronation to the vertical. Such a post theoretically mandates four degrees of motion that terminates with a vertical heel at the end of the first 25% of stance. An unposted device has no such mandate for motion and may not undergo the desired four to six degrees of motion at heel contact.
Rearfoot posts should be utilized with most functional orthotics to assure physiologic pronation as well as shock absorption. This is especially true for any foot that is maximally pronated at the moment of heel contact such as heel spur syndrome and sinus tarsi syndrome. In the latter case, a higher degree of motion may be desirable because the symptomatology is dependent on the impact of body weight onto an immobilized subtalar joint. Controlled motion is the best long-term therapy for this syndrome.
Written by Chris Smith, DPM, Former Vice President and Medical Director of Northwest Podiatric Laboratory and Professor Emeritus of Biomechanics at the California School of Podiatric Medicine (CSPM) at Samuel Merritt University.