RX GUIDE
Everything you need to
SUCCEED
Prescribe LIKE A PRO
Prescribing custom orthotics doesn’t need to be difficult – you just need the right partner. Whether you’ve worked with us for decades or are exploring a switch in custom orthotic labs, Northwest Podiatric Laboratory provides the knowledge, experience, and service podiatrists need to order custom orthotics with confidence.
SHELL/FOUNDATION
» = most commonly ordered options
Superglass®
Superglass orthotics include advanced fiberglass/graphite/epoxy resin components, a patented reinforcement system and a proprietary manufacturing technique. 1.5 mm thin no matter how rigid or flexible.
Flex
Thin and semi-flexible composite. For geriatrics and adults requiring control with a bit of flexibility.
»Everyday
A semi-rigid foundation – the perfect blend of control and flexibility to comfortably treat most patients.
Recommended for day-to-day use for most adults. Most-prescribed Superglass option.
Proformance®
Amazingly thin & rigid orthotics for serious athletes or patients who require a firmer device.
Recommended for athletes participating in activities like running, basketball, soccer, football or other high impact sports.
Polypropylene
Premium poly orthotics, the most popular material for custom orthotics featuring NWPL’s shape.
Maximum durability and amazing value.
Ideal for athletes, patients who are price conscious and/or applications where maximum durability is a must.
Semi-Flexible
Geared towards geriatrics and adults needing a bit more flexibility.
»Semi-rigid
Middle ground with both control and flexibility to comfortably treat most patients.
Recommended for day-to-day use for most adults.
Rigid
For very active and athletic patients who require a firmer device.
Recommended for patients participating in high impact sports.
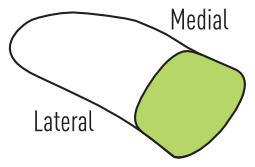
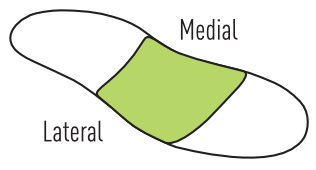
NCV®
NCV is a carbon fiber-reinforced engineered nylon.
Nearly as thin as Superglass, NCV strikes a balance between form, function and value.
Features softer medial and lateral edges for increased peripheral soft tissue accommodation. Approximately 2.5mm thin through the center and 1.5mm thin on the medial and lateral edges.
For patients who weigh 250 pounds or less.
Gentle
Comparable to Superglass Flex. Provides mild support along the long axis of the device.
For patients that require an orthotic that’s “forgiving” underfoot. Offers a high level of patient compliance.
»Firm
A hybrid between Superglass Flex and Superglass Everyday.
Semi-flexible support and a high degree of comfort.
Prescription Comfort®
Premium accommodative orthotics offering comfort and light control. A thin composite shell is built in so devices don’t lose their shape or “bottom out.”
With a maximum total thickness of 4.0mm, Prescription Comfort devices fit in nearly any shoe. A full-length (Complete) X-Guard on the plantar surface is standard.
Multi-Density
Our most accommodative orthotics featuring a very flexible composite shell with a layer of pre-stressed, dual-density foam. Add additional cushion as needed.
Ideal for diabetics or patients seeking maximum comfort.
»Composite
A hybrid between accommodative and functional orthotics with a flexible composite shell topped with a layer of pre-stressed foam. Add additional cushion as needed.
Ideal for treating diabetic, geriatric, pre/post-surgical patients and those with chronic foot disorders.
No top cover 
Shell material only – a custom orthotic in its purest form.
Pros: Same as ¾, plus: No top cover/cushion to wear out. Very high durability. Lower cost.
Cons: Same as ¾, plus: Can tear nylons. Can be more slippery.
3/4 
Extends from heel to end of orthotic shell. Can feature only a top cover (e.g. vinyl) or a cushion + top cover (e.g. soft EVA + vinyl).
Pros: Will fit in even the most low-profile shoes (dress, soccer cleats, etc.). Easy to move from shoe to shoe.
Cons: Limited accommodations. Exposes forefoot to the unfinished interior of the shoe. Less positional stability within the shoe.
To sulcus 
Begins at heel and ends proximal to the phalanges. Often requires additional forefoot cushion/extension. Infrequently prescribed.
Pros: Provides cushion for the met heads but allows for additional space in the toe box.
Cons: Drop off from the distal edge of the top cover to the inside of the shoe can be irritating for some patients.
»Heel to toe 
Extends the full length of the foot/inside of shoe. Often requires additional forefoot cushion/extension.
Pros: Helps keep orthotic properly positioned inside shoe. Is a direct replacement for the shoe insert. Allows for a full array of options/accommodations. Assists shock absorption for the forefoot.
Cons: Can cause shoe fit issues, depending on the shoe type and cover/cushion used. May be somewhat difficult to move from shoe to shoe. Forefoot/extension will eventually wear out.
»Vinyl
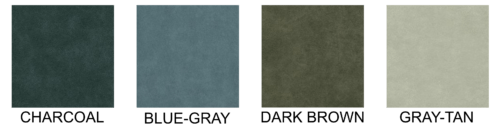
- •High quality synthetic leather.
- •Top cover only.
Pros:
- •Durable with a long lifespan.
- •Very similar in appearance to leather.
- •Available in four colors (charcoal, dark brown, gray-tan and blue-gray).
Cons:
- •Not breathable.
- •Can feel “slippery” to some patients.
- •Can curl and crack over time.
Common uses:
- •Everyday orthotics for most patients.
- •When durability is important (children, teenagers, work boots, etc.)
Leather
- •Natural leather with light grain.
- •Top cover only.
Pros:
- •Luxurious feel.
- •Durable.
- •Complements high end shoes.
Cons:
- •Can bleed, discolor and/or smell.
- •Cost.
Common uses:
- •When aesthetics are important (e.g. sandals, dress shoes, high heels, etc.).
- •Patients with allergies to man-made materials.
Microsuede
- •High-end synthetic suede fabric from a leading manufacturer.
- •Top cover only.
Pros:
- •Feels great under foot.
- •Not slippery.
- •Breathability.
- •Color won’t bleed.
Cons:
- •Can “grip” patients’ socks
- •Will eventually lose its soft, plush feel.
Common uses:
- •Excellent alternative to vinyl.
Neoprene
- •Synthetic rubber (1/16″ or 1/8″) with a fine weave cloth top layer.
- •Top cover + cushion combination.
Pros:
- •Top cover and cushion in one.
- •Good feel under foot.
- •Some breathability.
Cons:
- •Less durable than vinyl.
- •Can hold odors.
Common uses:
- •Athletic devices.
»Firm EVA
- •Low density, closed-cell EVA foam (1/16″ or 1/8″).
- •Cushion/extension or top cover.
Pros:
- •Very durable.
- •Won’t absorb perspiration.
- •Excellent shock absorption.
- •Molds slightly to the foot, but “rebounds” when not in use.
Cons:
- •Not a “soft” material.
Common uses:
- •Great all-purpose cushion material.
- •Most functional orthotics.
Soft EVA
- •Closed-cell EVA foam (1/16″ or 1/8″).
- •Cushion/extension or top cover.
Pros:
- •Compresses and molds to the foot.
- •More durable than popularly prescribed Plastazote .
Cons:
- •Can “bottom out”.
- •Can abrade or wear out more quickly than other materials.
Common uses:
- •Accommodative orthotics.
- •Geriatric patients.
Diabetics.
P-Foam
- •Extra soft, memory foam-like cushion.
- •Popular, orthotic-grade urethane foam (1/16″ or 1/8″).
- •Cushion/extension only.
Pros:
- •Great combo of softness & durability.
- •Widely used with long track record.
Cons:
- •Bottoms out somewhat quickly.
- •Can abrade or wear out more quickly than other materials.
- •Tears easily.
Common uses:
- •Accommodative devices.
- •Extra comfort for functional devices.
Arch height
»Standard (default)
Leaves some space between the patient’s arch and the medial arch of the orthotic for foot elongation during gait.
High or very high
The orthotic is more intimate with the patient’s foot and may appear to have a more “custom” or exact fit. Can cause arch pain for some patients.
Low
More comfortable for some patients but may allow for overpronation.
»X-Guard (bottom cover)
Adds durability by reinforcing the transition between the orthotic shell and extension. Aesthetically pleasing.
POSTING
»Heel post
Crafted from a proprietary material that slightly compresses and rebounds with each step.
- •Flat/vertical: Immobilizes the subtalar joint at the moment of heel contact and attempts to maintain the calcaneus in a vertical position. For tarsal coalitions, flat feet associated with muscle spasm or any time that the prime concern is stability.
- • Varus: Is generally 4 degrees but could be 6 degrees (rarely more). This places the heel 4 (or 6) degrees inverted at heel contact and permits the calcaneus to evert to perpendicular. The post mandates motion in the subtalar joint for normal locomotion.
Integrated heel post
Heel post built into the orthotic shell.
- • Polypropylene only. No additional charge.
Heel lift
A heel lift decreases the tension on the Achilles tendon and reduces the pronatory force of the foot. Heel lifts greater than 1/8” can raise the heel out of the shoe.
Heel lifts of up to 1/2” are available to correct limb-length discrepancy.
Forefoot post
Crafted from a proprietary material that slightly compresses and rebounds with each step.
Extrinsic forefoot posting controls the foot better than intrinsic forefoot correction. However, extrinsic forefoot posting requires increased shoe volume and can be destructive to the shoe.
Keep extrinsic posting no more than 3 to 4 degrees. Further correction should be intrinsic.
Integrated forefoot post
Heel post built into the orthotic shell.
- • Polypropylene only. No additional charge.
HEEL
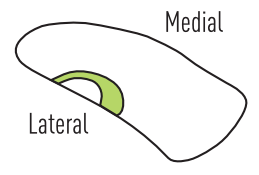
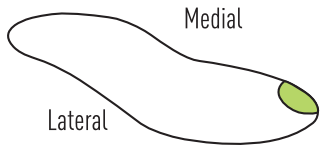
»Deep heel cup
More fully encapsulates the plantar, lateral, medial and posterior aspects of the heel. Adds lateral stability and reduces heel pain (increases weight-bearing area and decreases direct pressure). Can help stabilize foot on the orthotic.
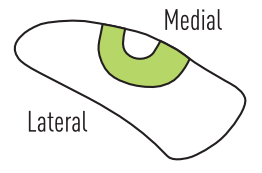
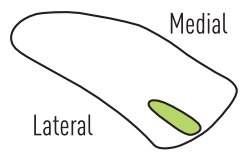
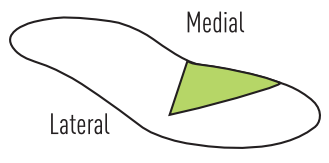
»Medial heel skive (Kirby skive)
Flat area on medial aspect of heel cup (intrinsic varus wedge). Increases the supinatory force to the subtalar joint. Often used with a heel post for increased stability.
Donut cushion
»Heel cushion
Horseshoe cushion
Medial accommodation
In shell or in cushion
ARCH/MIDFOOT
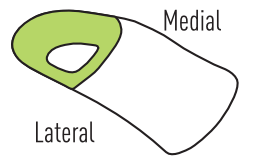
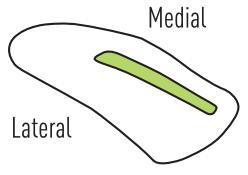
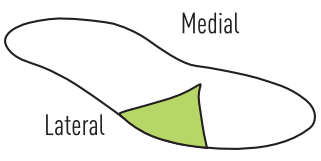
»High medial overlay
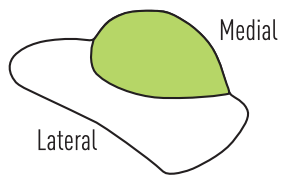
Like scaphoid pad, but pad extends past the medial edge of the shell. Can help prevent medial edge of the orthotic from digging into the medial arch of the foot.
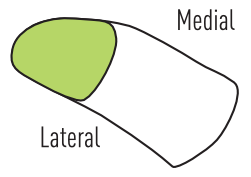
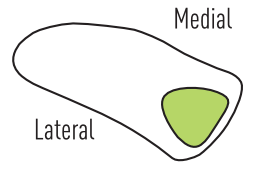
Scaphoid pad
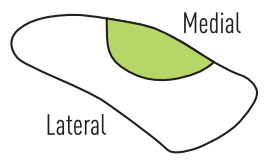
Supports the talonavicular joint, decreasing the medial displacement of the midfoot. Pad ends at medial edge of shell.
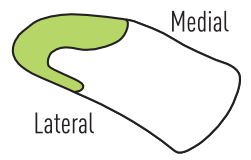
Flatten plantar medial
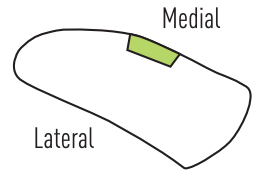
Flattens medial border of shell only. Forms a flatter lip on the high point of the arch. More comfortable for high arches.
Base of 5th/styloid (In shell or pad)
Cuboid accommodation (In shell or pad)
Navicular accommodation (In shell or pad)
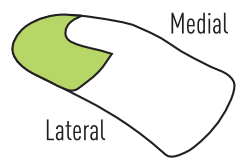
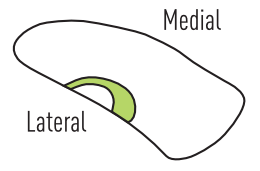
Plantar fascia accommodation
Linear channel in the shell or cushion underlying the medial slip of the plantar fascia. In shell or in cushion.
High medial/ high lateral
High flanges on medial and lateral aspect of shell. Increases control of rearfoot/midfoot. Potential for irritation on high medial.
METATARSAL
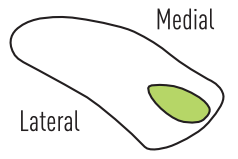
»Cutouts
Available in shell or in cushion. Reduces weight-bearing, providing a sweet spot for met heads 1 to 5.
»Met pad
Available in soft and firm. Firm is default.
Full met pad
Pad to support metatarsal arch; provides offloading of met heads and increase loading of met shafts.
Met raise (in shell)
Same as a met pad, but in shell. Generally lower than a met pad as it can cause pain if too high or too distal.
»Dancer’s pad
Pad across distal 1/3 of met shafts to base of toes. Allows for cutouts to offload a given metatarsal.
Neuroma pad
Shaft pad
FOREFOOT
Forefoot wedge
Wedge shaped extension from distal end of shell to toes. Provides inversion or eversion positioning on foot after heel raise. A less aggressive alternative to a forefoot post.
Morton’s extension
Soft in-cushion extension limits motion. Rigid in-shell extension prevents motion at 1st MTPJ.
Reverse Morton’s extension

Allows the 1st metatarsal to plantarflex below the plane of the lesser metatarsals, thereby relatively increasing the dorsiflexion available at the 1st MTPJ. Useful for hallux limitus/DJD of the 1st MTPJ.
Hallux accommodation
Toe crest accommodation
Everyday
- •Most popular configuration for patients with average activity level and general foot pain.
- •Designed to fit in nearly any type of footwear.
- •Add a heel post if extra lateral stability is desired.
Dress
- •Heel below 1.5″ – Slightly narrower design with softer cushion and more luxurious top cover.
- •Heel above 1.5″ – Extra narrow design. Only 1.1mm thin. For heels 1.5″ to 4.0″. Restores natural balance.
Athletic
- •”Low profile shoes” – For lower-volume shoes where space for an orthotic is limited (soccer cleats, sleek running shoes, etc.).
- •”Standard/high profile shoes” – For standard/high volume shoes (e.g. traditional running shoes, basketball shoes, etc.). Blend of firm support and shock absorption for high impact activities.
- •”Standard/high profile shoes + stability” – Same as “standard/high profile shoes” with the addition of a heel post for additional lateral stability. Adds minimal bulk, but may cause heel to “pop out” of some shoes.
Amputee
- •Utilizes custom-shaped foam to replace missing toes or portions of patient’s foot.
- •Orthotic features moderately flexible shell and multiple layers of foam to provide support and decrease irritation and hot spots.
Achilles tendinitis
- •Superglass Everyday.
- •Deep heel cup with high lateral flange.
- •Heel post (consider heel lift, bilateral).
Ataxic gait
- •Very deep heel cup.
- •Vertical forefoot post.
- •Vertical rearfoot post.
- •Forefoot extension (full).
Bunion/hallux valgus
- •Superglass Everyday.
- •Heel post.
- •Reverse Morton’s extension.
Charcot-Marie-Tooth
- •Superglass Proformance.
- •Forefoot post with 3 or 4 degrees of correction (remaining correction intrinsic).
- •Vertical heel post.
Hallux rigidus
Morton’s extension (in device) with additional dorsiflexion.
Plantarflexed first ray
- •Cutout, 1st (in-cushion).
- •Reverse Morton’s extension.
Rigid cavus foot
- •Flatten plantar medial.
- •Correct first four degrees of valgus extrinsically and correct the remainder intrinsically.
Shin splints
- •Superglass Everyday.
- •Deep heel cup.
- •High medial overlay or scaphoid pad.
Questions about prescribing custom orthotics? Contact Customer Care for an in-depth walk through of the Custom Orthotic Prescription Guide and ordering options.